


 Fiona McMahon PT, DPT & Jessica Babich PT, DPT Fiona: Hello everyone, for those of you who didn’t get a chance to catch my blog a few weeks back, Beyond Basics Physical Therapy is joining forces with the Tisch Multiple Sclerosis Research Center of New York to raise money to support multiple sclerosis research, through Team Tisch MS NYC, in this year’s New York City Marathon. Our goal is $2,500 and WE ARE SO CLOSE, if you care to donate, please click here. I will be running the marathon in November, and Beyond Basics Physical Therapy is working to support my fundraising endeavors as well as showing the running community the invaluable benefits of having a sharp, perceptive, thorough and expert physical therapist on your side during training; and that goes for ANY sports training! I just had my first evaluation with Jessica Babich, PT, DPT, who is both a pelvic floor physical therapy expert as well as a functional movement specialist with an extensive background in orthopedics and sports-related injuries. Jessica was super thorough, she took an extremely detailed history, she looked at my posture, joint mobility and mechanics, strength, core function, and even how my shoes were constructed to see if they were good enough to run in! The shoe part was super wild! In this blog you will see where I stand from a physical therapy perspective, and where I hope to go. Both Jessica and I are authors in this blog so keep an eye on who is talking so you can get the full scoop from both the physical therapist and the patient perspective
Fiona McMahon PT, DPT & Jessica Babich PT, DPT Fiona: Hello everyone, for those of you who didn’t get a chance to catch my blog a few weeks back, Beyond Basics Physical Therapy is joining forces with the Tisch Multiple Sclerosis Research Center of New York to raise money to support multiple sclerosis research, through Team Tisch MS NYC, in this year’s New York City Marathon. Our goal is $2,500 and WE ARE SO CLOSE, if you care to donate, please click here. I will be running the marathon in November, and Beyond Basics Physical Therapy is working to support my fundraising endeavors as well as showing the running community the invaluable benefits of having a sharp, perceptive, thorough and expert physical therapist on your side during training; and that goes for ANY sports training! I just had my first evaluation with Jessica Babich, PT, DPT, who is both a pelvic floor physical therapy expert as well as a functional movement specialist with an extensive background in orthopedics and sports-related injuries. Jessica was super thorough, she took an extremely detailed history, she looked at my posture, joint mobility and mechanics, strength, core function, and even how my shoes were constructed to see if they were good enough to run in! The shoe part was super wild! In this blog you will see where I stand from a physical therapy perspective, and where I hope to go. Both Jessica and I are authors in this blog so keep an eye on who is talking so you can get the full scoop from both the physical therapist and the patient perspective 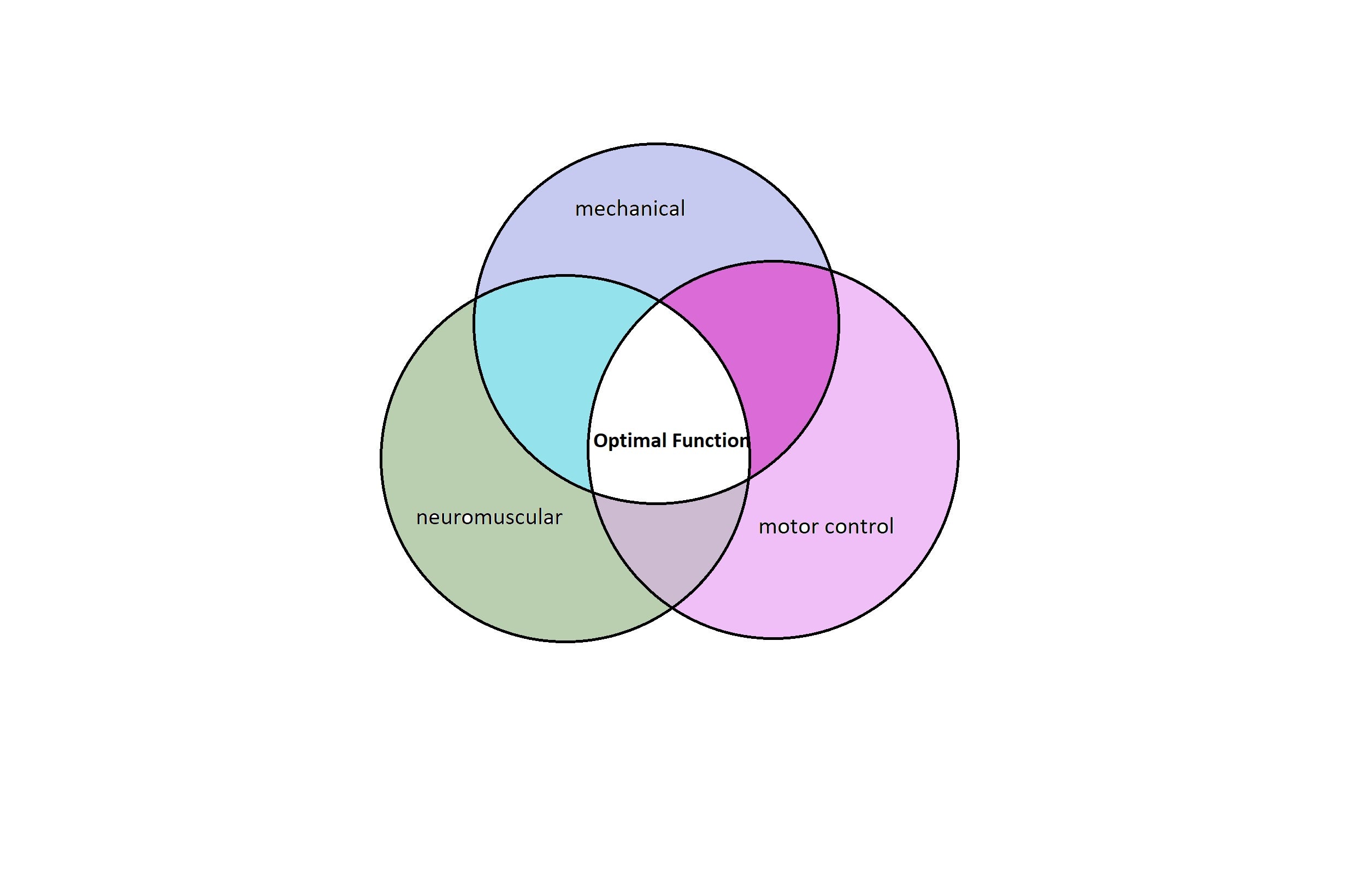 Jessica: When I look at runners, I first assess the individual as a whole and identify which area in their body seems to be driving inefficiency. I look at the 3 pillars of functional efficiency, (Mechanical, Neuromuscular, and Motor Control) when examining my patients. Within the mechanical capacity, I examine which structures such as joints, muscles, viscera, neurovasculature, etc., that could inhibit optimal functional performance. Specifically with a runner, I am interested in his or her alignment as well as range of motion through their rib cage, spine, pelvis, and lower extremities. Looking at a patient’s posture in both walking and running, allows me to determine the momentum driving the patient forward. This can be helpful in finding out what and where a dysfunction may be that could affect a runner’s performance. With a runner, I am interested in how he or she initiates his or her run. Are they able to drive force through their lower extremities into their trunk without spinal compensation. Does the runner have adequate strength and endurance to maintain appropriate form and movement strategy throughout their run? I also examine what happens to the patient’s form during walking when you slow him or her down. Breaking down the whole movement pattern and looking at individual parts helps to further expose any problem areas. I examine dynamic stability and controlled mobility to ensure my patients are moving efficiently. From there, I examine the basics, is there a lack of movement (is something stuck or tight) that can affect a runner’s ability to powerfully push off the ground when they run and absorb force when they land. Lastly, I am evaluating Motor Control. If the mechanical capacity and neuromuscular function is present, how does this individual choose to move, or what is his or her strategy to get from point A to point B. This is where a lot of the training comes into play. History Fiona: I told Jessica about my previous injuries, almost all have occurred secondary to decades of running (It truly is my favorite activity), currently I am feeling some left sciatic pain, which has become fairly bothersome. .Orthopedic Injuries
Jessica: When I look at runners, I first assess the individual as a whole and identify which area in their body seems to be driving inefficiency. I look at the 3 pillars of functional efficiency, (Mechanical, Neuromuscular, and Motor Control) when examining my patients. Within the mechanical capacity, I examine which structures such as joints, muscles, viscera, neurovasculature, etc., that could inhibit optimal functional performance. Specifically with a runner, I am interested in his or her alignment as well as range of motion through their rib cage, spine, pelvis, and lower extremities. Looking at a patient’s posture in both walking and running, allows me to determine the momentum driving the patient forward. This can be helpful in finding out what and where a dysfunction may be that could affect a runner’s performance. With a runner, I am interested in how he or she initiates his or her run. Are they able to drive force through their lower extremities into their trunk without spinal compensation. Does the runner have adequate strength and endurance to maintain appropriate form and movement strategy throughout their run? I also examine what happens to the patient’s form during walking when you slow him or her down. Breaking down the whole movement pattern and looking at individual parts helps to further expose any problem areas. I examine dynamic stability and controlled mobility to ensure my patients are moving efficiently. From there, I examine the basics, is there a lack of movement (is something stuck or tight) that can affect a runner’s ability to powerfully push off the ground when they run and absorb force when they land. Lastly, I am evaluating Motor Control. If the mechanical capacity and neuromuscular function is present, how does this individual choose to move, or what is his or her strategy to get from point A to point B. This is where a lot of the training comes into play. History Fiona: I told Jessica about my previous injuries, almost all have occurred secondary to decades of running (It truly is my favorite activity), currently I am feeling some left sciatic pain, which has become fairly bothersome. .Orthopedic Injuries
- Right hip labral tear
- Right knee pain (patellofemoral pain syndrome), which comes and goes but is currently under control
- Occasional left knee pain (patellofemoral pain syndrome), much less bothersome than the right side
- Mild to moderate left calf pain, which also comes and goes
- Right ankle sprain, from a failed handstand (don’t ask), no longer bothersome, but not properly rehabbed
Medical
- Largely unremarkable, neural tension secondary to Arnold Chiari Type I malformation. Chiari occurs when part of the brain (the cerebellum) herniates through the skull opening into the spinal cord. It sounds pretty awful, but for me, it’s not too bad and I only experience occasional dizziness as a symptom.
Current Exercise Routine:
Get help now from a pelvic floor therapist
- I’m pretty regimented and break most of my workouts into 2 daily sessions. I run in the morning, currently I am working on speed training and run something between 3 and 8 miles daily, 5-6 times weekly. I am following one of my favorite marathon gurus, Hal Higdon’s plan, which you can see for yourself here. I have used Hal’s plans for 2 of the 4 previous marathons I’ve run, and I really like how he organizes his plans. I would advise anyone thinking of trying a marathon, to use a training plan. It allows you to ease yourself gently into upping the mileage, rather than panicking at 5 weeks before the race that you haven’t taken your long runs over 20 miles. Following my run I do a mixture of stretches, use my stick ( it’s like a foam roller) and a trigger point ball to roll out my muscles. 4 nights a week I do PM weightlifting sessions, which last about 40 minutes. I split my lift into upper body and lower. I do a mixture of stabilizing and traditional exercise. When I’m done I’ll stretch again and this time roll out on a foam roller. In order to support all that exercise I drink a ton of water and try and fill my diet with lots of whole grain carbs, lean protein, and healthy fats (I’m looking at you avocados!)
The Evaluation: Posture:
 Jessica examining my posture and my ability to tolerate load through the spine using the Vertical Compression Test
Jessica examining my posture and my ability to tolerate load through the spine using the Vertical Compression TestFiona has a posterior/posterior alignment. ( This terminology comes from the Institute of Physical Art (IPA), and is a wonderful training program for PTs) Meaning, her ribcage is set posterior in relationship to her pelvis and her ribcage is tipped posteriorly. Range of Motion (ROM):
-
Poor lumbar spine ROM, with an inability to reverse the curve in my lumbar spine
- Why this is important: my spine should have motion in order to absorb the shock from repeated foot falls, also an immobile spine may inhibit the core stabilizers from firing properly
-
HISL testing ( another IPA test): Positive at the right (hip) at 90 degrees, with poor glide of the femur down on the left side. Positive at left (hip) at 100 degrees.
- How do we translate this into non-physical therapy speak? First of all the HISL stands for Hip, Innominate, Sacrum, and Lumbar. It measures the relationship between the bones of the upper thigh, pelvis, and low back. What my results tell us is that my hips are stuck and cause my innominate (bone in the pelvis) to move too early. This is not so great because it causes the bones further up to have to move extra to compensate. We have to clean this up.
Strength and Function :
- Instead of testing muscles one-by- one, which is commonly done in traditional physical therapy practices, we decided to take a look at functional movements. Who gives a hoot if I have strong quadriceps while sitting on an exam table, if they can’t function properly during actual running, right?
-
LPM (Lumbar Protective Mechanism)( another IPA test) : absent in all quadrants
- Dang! Lumbar protective mechanisms refers to the ability to stabilize your spine and protect your core in response to bumps and jostles. I didn’t stabilize at all. This is important because running is essentially a series of bumps and jostles, running on an unstable spine and core can increase your chances of injury as well as reduce your power during push-off in running leading to slower times (HORRENDOUS!).
- Sagittal Plane Lunge: I have deficits with initiation and weight acceptance on both sides. I compress my arms in prayer position to create stability and when taken away I have a loss of trunk control. My right ankle more unstable than the left.
-
Runner’s Start Jump: difficulty coordinating movement on both sides, but significantly worse with initiation from right side at the ankle.
- Remember my ankle sprain? Well, apparently that’s still holding me back and decreasing my ability to push off the ground. You could imagine how this could become a problem over the course of 26.2 miles. Moral of the story, see a PT after you hurt your ankle!
- Also we see deficits in core control again. I think addressing this with Jessica will really improve my time.
Shoes and wear:
- Apparently my shoes were good! Jessica told me that sometimes right and left sneakers can be made in different factories and have different densities, which can really mess you up while running. Also if the back part of you sneaker extends too far it can make your brain think your foot is larger than it is, leading to injury. The wear of the shoe is also important to see if one foot pronates or supinates more than the other. If this was the case, Jessica could work on the alignment of the bones in my feet, ankle and foot strength, as well as teaching me how to tie my shoes in a way that better support my feet.
Assessment and Take Away: Jessica’s Assessment: Fiona, like a majority of our athletes presents with deficits in the 3 major pillars leading to functional inefficiency. The goal of physical therapy, isn’t always to reduce pain, it is to get you to function better, which in turn will decrease wear and tear that contribute to common pain patterns. Fiona: I can’t say I am surprised by much of what we found. I am slightly disappointed with my core activation finding, because I had been focusing on that particular issue for months and months in the gym. Jessica told me she thought part of my issue was that my lower (lumbar) spine was so rigid, it might be hard for me to get into a place where my deep core muscles can work to facilitate stability. It goes to show, even as a physical therapist, you need someone else to literally watch your back. As a physical therapist, my evaluation showed me that now is the time for help. Although I am strong and spend hours working out, my core stability is something I need more help with, and I simply cannot work my way out of my weakness alone in a gym. I’ve tried long enough. I need gentle manual therapy and proprioceptive neuromuscular feedback to wake my lazy deep stabilizers out of their hibernation and orthopedic work to allow the joints of my spine and pelvis to move more efficiently and effectively. Although this body has its deficits, I’m really proud of what it has done so far, and I’m really excited to see where Jessica will help me go! Plan:
- Improve the movement of: right foot, trunk, and cervical spine
-
Improve core stability and strength to allow for more power and reduction of injury risk
- We will achieve these goals through manual work, neuromuscular re-education in order to teach the muscles to activate better and a strong home program to maintain changes made in physical therapy.
Goals Jessica: My goal is to treat the mechanical deficits inhibiting her neuromuscular system and then functionally reintegrate the parts into the whole system to enhance performance efficiency. Long Term Goals:
- 1: (12 Weeks) | Patient to demonstrate core first strategy with transitional movements to improve stability, energy efficiency and decrease risk for injury
- 2: (12 Weeks) | Patient to demonstrate optimal ribcage over pelvic posturing for automatic core engagement and decrease mechanical load on system.
- 3: (12 Weeks) | Patient to improve R foot positioning for stability and push off in gait
Home Exercise Program: So far I have one addition to my workout routine. It is a split stance at the wall designed to wake up my stabilizers before I go running. I stand at the wall with one leg fully extended on my toes and the other bent at the knee and the hip, with my toes pointed up. I hold for 30 seconds per side and then I get going. It has been a couple days since this exercise was assigned, and I’ve done it on about 50% of my runs. Remembering to do your home program is one of the biggest challenges of physical therapy. My strategy to combat this is to leave a sticky note on my door reminding me before I leave the house. I will report back on future blogs to let you know how my strategy worked out. That’s it for now: Check out more info and pictures on our instagram and facebook pages Click Here to Donate to support Team Tisch MS NYC:
