


You’re feeling good and the body is flowing at the yoga studio or in the bedroom… then a sound comes out of your vagina. What was that?! Queef, vart, vaginal wind, vaginal air, vaginal flatus, vaginal gas, chattering vulva, fanny fart, garrulitas vulvae, flatus vaginalis, incontinentia vulvae, and noisy vagina all describe the involuntary passing of trapped odorless gas from the vagina.
Occasional vaginal noise from trapped air is natural and normal… it is air moving. While vaginal gas is common, the experience can still be embarrassing, isolating, and impact quality of life. Unless vaginal wind has an odor, vaginal flatus does not require medical attention. However, you should share this symptom with your medical professional if vaginal sounds bother or worry you. Frequent vaginal wind may suggest poor regulation of pressure in the vaginal pelvic cavity between the abdomen and pelvic floor and may be improved when addressing some contributing factors. Vaginal delivery and pelvic floor disorders increases the likelihood of vaginal flatus. In a group of women with pelvic floor disorders, 35% of women reported vaginal gas, especially those with younger age, increased sexual activity, worsened sexual function, more severe urinary or stool leakage, and lack of menopausal symptoms.
What makes that sound?
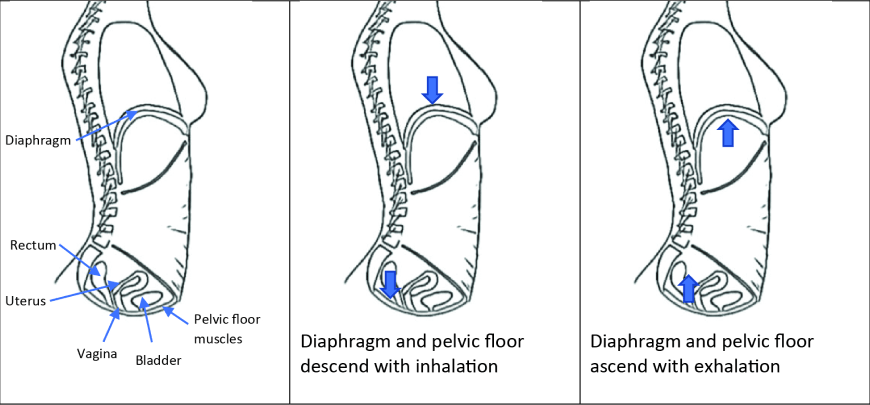
The vagina makes sounds when air moves rapidly through the opening with pressure changes from the top, around, within, or the bottom of the vagina. The vaginal canal connects the vulvar opening at the bottom and the uterine cervix at the top. The walls of the vagina move with pelvic and abdominal organs and changes of abdominal pressure. With balanced abdominal and vaginal pressure and strong pelvic floor closure, air regularly moves in and out of the vaginal opening silently. Vaginal sounds are more difficult to control than around the anus because vaginal muscles do not close as tightly.
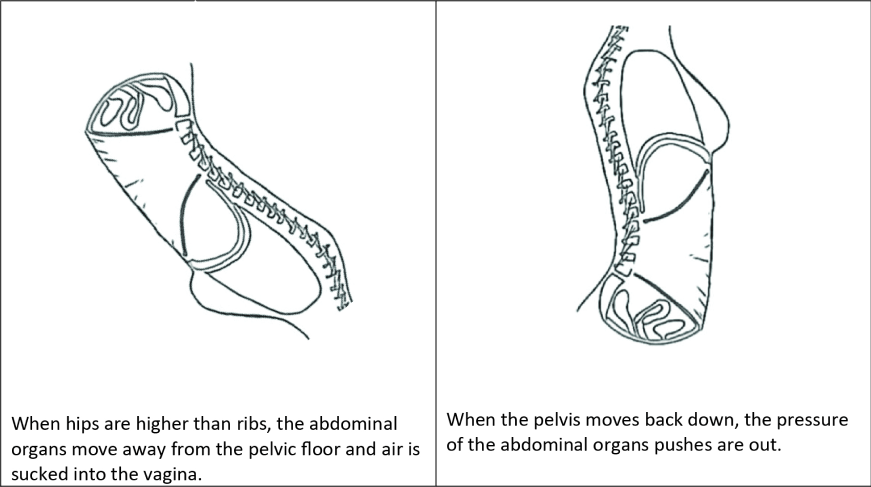
 Vaginal noise commonly occurs with pressure changes from penetration or pressure from the bottom of the vagina. Penetration occurs with sexual intercourse, gynecological exams, tampon or menstrual cup insertion. Pressure at the bottom of the vagina happens when the pelvis is higher than the abdomen. The pressure outside of the vagina and gravity can move pelvic floor muscles into the vagina, especially with pelvic floor dysfunction. Stretching overactive pelvic floor muscles in positions like downward dog or legs wide allows air in and then air pushes out when the pelvic floor returns to its resting state. Underactive pelvic floor muscles with increased movement air in and out of vagina with relative weakness of pelvic floor muscles and loose vaginal entry.
Vaginal noise commonly occurs with pressure changes from penetration or pressure from the bottom of the vagina. Penetration occurs with sexual intercourse, gynecological exams, tampon or menstrual cup insertion. Pressure at the bottom of the vagina happens when the pelvis is higher than the abdomen. The pressure outside of the vagina and gravity can move pelvic floor muscles into the vagina, especially with pelvic floor dysfunction. Stretching overactive pelvic floor muscles in positions like downward dog or legs wide allows air in and then air pushes out when the pelvic floor returns to its resting state. Underactive pelvic floor muscles with increased movement air in and out of vagina with relative weakness of pelvic floor muscles and loose vaginal entry.
Pressure changes from the top of the vagina occur with abdominal and pelvic organ movement with changes in position and stabilization patterns. This happens with positions of pelvis higher than ribs in yoga and other exercises, some prayer postures, getting up off the floor, and in some positions for intercourse. Abdominal stabilization exercises, breath holding, and variations in vocalizations also increase pressure into the vagina and air flow.
Get help now from a pelvic floor therapist
The vagina is lined with folded expandable tissue that allows for penetration, babies, blood flow, and air. Pockets of air can get trapped in the vaginal folds and ridges. Excessive pressure changes within the vagina occur when pelvic organs relax into the vaginal walls or when the diaphragm and pelvic floor move opposite of each other. Rigid vaginal walls, specifically after radiation or disease, can also increase vaginal noise because of increased space in the vagina and decreased moderation with changes in air flow.
The degree of vulvar and vaginal moisture and lubrication affects vaginal noise. Changes in the moisture of the folds of the vaginal walls controls how much air is trapped and how air moves. The lips (labia) of the vulva require sufficient lubrication to close the introitus to limit air flow in and out. While lubrication helps seal the vagina, increased moisture also augments noise when air does move. This may be one of the reasons why age decreases the frequency of vaginal sounds.
Pelvic organ movement or variations of the uterus also changes pressure at the top and into the vagina. Pelvic organ movement can be a temporary hormonal or progressive laxity of pelvic organs leading to prolapse. Hormones fluctuate monthly, around childbirth, and around menopause. 47-66% patients with pelvic organ prolapse report vaginal flatus compared to 27% for patients with stress urinary incontinence. Variations in uterine position and conditions such as a retroverted uterus or after uterine removal also alters vaginal pressure.
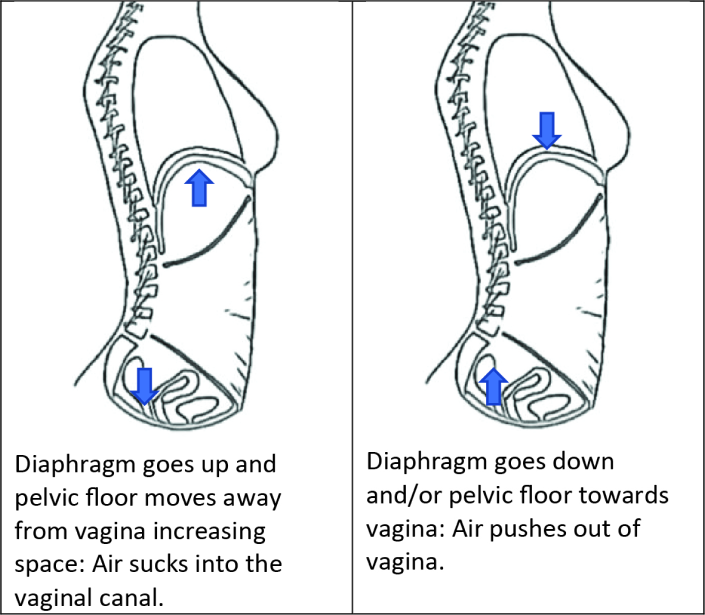
When the pelvic floor and diaphragm move in opposite direction, this change in pressure pulls or pushes air out of the vagina. Air pulls into the vagina when the pelvic floor elevates while the diaphragm is low during an exhale. Air pushes out of the vagina when the pelvic floor drops while the diaphragm is high during exhale or with the movement of organs. This happens when breathing patterns are not synchronized between the pelvic floor and abdominals or when a task is particularly difficult.

What to do about it?
Until pelvic noises become accepted in society, many people will want to minimize the frequency and intensity of vaginal wind. Vaginal sounds can partially modified decreasing trapped air and limiting the rapid changes in vaginal pressure by:
- Using a tampon or pessary. This works by limited the amount of air in the vagina and decreasing the movement of the pelvic organs into the vagina
- Improving the closure of the vaginal opening with:
- Pelvic floor strengthening includes the contraction, relaxation, and coordination of the pelvic floor muscles. Pelvic floor muscle training is rarely prescribed in isolation and instead incorporated as part of a more comprehensive approach that is individualized for the patient’s problems, lifestyle demands, and goals. As a general prescription, pelvic floor muscle training for strengthening comprises of:
- 3 sets of 8 almost maximum pelvic floor contractions held for 8 seconds every day
- Using the cue to close and lift the vaginal opening as if to stop urine mid- stream (but not actually doing this while urinating)
- Making sure to relax between contractions and not hold the breath
- Hormonal creams or vaginal moisturizers
- At the vulvar lips, increasing the moisture helps to improve the closure of the introitus to limit excessive air flow.
- Within the vagina, improving moisture decreases the amount of air that moves.
- Coordinating abdominal pressure to decrease abdominal organ movement when hips are above ribs
- Keep breathing.
- For overactive pelvic floor muscles:
- Inhale to keep space in at the pelvic floor
- Then move
- For underactive pelvic floor muscles:
- Inhale to open pelvic floor
- Exhale to engage pelvic floor and abdominals for stability
- Then keep exhaling while moving
- During penetration, decreasing the speed and depth of initial entry
- General abdominal pressure management:
- Functional activity training adjusts breath patterns, posture, muscle patterns to breath holding and downward pressure.
- Julie Wiebe, a highly regarded clinician and researcher, gives an easy cue, “blow before you go,” to help manage excessive downward pressure and encourage pelvic floor support.
- When breath holding becomes the primary stabilization pattern, exhale before and during the most difficult part of exercise.
Vaginas are cool. They change through the lifetime, allow and prevent things entering and exiting, adapt for sensation, self-clean, and yes, make noise. For most people, vaginal sounds do not require additional attention. For some people, a pelvic floor physical therapist can help improve the factors to decrease bothersome vaginal flatulence. At Beyond Basics Physical Therapy, we can help diagnose and treat the underlying causes for pelvic floor dysfunction.
REFERENCES:
- Lau HH, Su TH, Chen YY, Huang WC. The Prevalence of Vaginal Flatus in Women With Pelvic Floor Disorders and Its Impact on Sexual Function. The Journal of Sexual Medicine. 2021 Mar 1;18(3):487-92.
- Miranne JM, Marek TM, Mete M, Iglesia CB. Prevalence and resolution of auditory passage of vaginal air in women with pelvic floor disorders. Obstetrics & Gynecology. 2015 Jul 1;126(1):136-43.
- Neels H, Mortiers X, de Graaf S, Tjalma WA, De Wachter S, Vermandel A. Vaginal wind: A literature review. European Journal of Obstetrics & Gynecology and Reproductive Biology. 2017 Jul 1;214:97-103.
- Neels H, Pacquée S, Shek KL, Gillor M, Caudwell-Hall J, Dietz HP. Is vaginal flatus related to pelvic floor functional anatomy?. International Urogynecology Journal. 2020 Dec;31(12):2551- 5.
- Pool-Goudzwaard AL, Eijkemans MJ, Steegers-Theunissen RP, Burger CW, Vierhout ME. Vaginal noise: prevalence, bother and risk factors in a general female population aged 45–85 years. International Urogynecology Journal. 2009 Aug;20(8):905-11.
- Sahar T, Fatemeh M, Parvin B, Reza SM. The Comparison of the Effects of Pessary, Pelvic Floor Physiotherapy, and Corrective Surgery Methods in Correction of Vaginal Sound in Patients with Pelvic Floor Disorders
- Schorno-Pitsch A. Vaginal farting or queefing: tips to decrease your personal symphony. Core Exercise Solutions. https://www.coreexercisesolutions.com-tips-to-stop-vaginal-farting-or-queefing/ Accessed on: May 1, 2022. Published on April 11, 2019.
